

Mulgrew Lied Again: How the UFT and City Sold Members on a “No-Tiering” Plan Built on - Guess What? Tiering.
The latest Mulgrew lie: There's no tiering in this plan. / The truth: The original plan was always the three tiers in the present plan, with Tier 1 being zero dollar copays, since at least 2018.

They told us there is no tiering in this new plan. The 2018 internal City documents say otherwise.
When UFT and Municipal Labor Committee (MLC) leaders promoted the new NYCE PPO healthcare plan, they assured members:
“There is no tiering of hospitals in the NYCE PPO.”
But buried in internal City documents, consultant reports, and even the UFT’s own fine print lies the truth: Tiering has always been part of the plan for cost savings.
This isn’t new. It’s the continuation of a long-term blueprint — one that began years ago under the guise of “cost savings” and “preferred networks.”
And now, with United Healthcare’s UMR and Emblem at the center of a new self-funded system, that blueprint is being quietly activated.
The “No-Tiering” Promise That Isn’t
In the UFT’s official FAQ (see image below), the union writes:
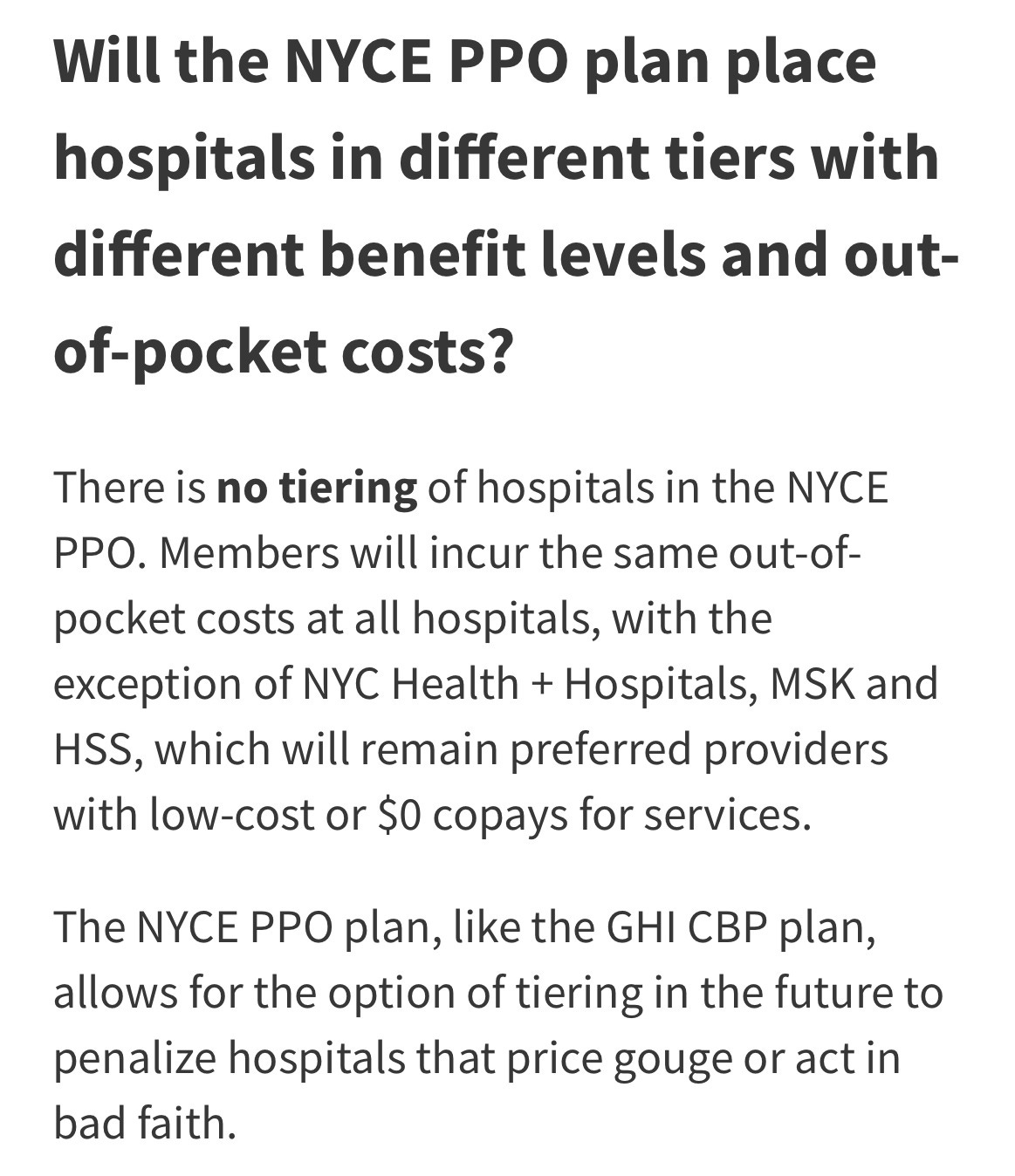
Will the NYCE PPO plan place hospitals in different tiers with different benefit levels and out-of-pocket costs?
“There is no tiering of hospitals in the NYCE PPO. Members will incur the same out-of-pocket costs at all hospitals, with the exception of NYC Health + Hospitals, MSK and HSS…”
”The NYCE PPO plan, like the GHI CBP plan, allows for the option of tiering in the future to penalize hospitals that price gouge or act in bad faith.”
Translation: “No tiering — for now.”
This is deliberate rhetorical framing: deny change, then quietly permit it.
It’s the same playbook used for co-pay increases and preauthorization changes — soften resistance now, implement later once members are locked in.
The Smoking Gun: The City’s 2018 “Menu of Savings” Memo
Five years before this plan’s rollout, the City’s Office of Labor Relations (OLR) and its provider vendors — Empire BlueCross and EmblemHealth — were already designing a three-tier hospital and provider system while collaborating with the MLC to implement it for January, 2019.
The February 8, 2018 memo, “Re: Questions on Menu of Savings”, sent by the UFT’s Arthur Pepper, in his role in the MLC’s Technical Committee, to the City’s Office of Labor of Relations makes the intent crystal clear:
“The starting point appears to also include plan design changes to the current plan. When this was initially discussed with Empire, Tier I would cost nothing to members, Tier II would cost the same copays that exist today, and Tier III would cost something substantially more.”
Sound familiar? That’s because that is exactly the framework we have now with the NYCEPPO plan.
It goes further, mapping the structure in detail as to what it may look like for the existing GHI-CBP plan:
“Visits to PCPs affiliated primarily with the City’s Health + Hospitals system will be subject to $0 copay per visit (Tier 1 Medical Provider).
Visits to PCPs affiliated primarily with hospitals designated as the City’s Tier 2 hospital network will be subject to a $15 copay per visit. (Tier 2 Medical Provider)
Visits to PCPs affiliated with hospitals designated as the City’s Tier 3 hospital network will be subject to a $30 copay per visit. (Tier 3 Medical Provider)
Visits to PCPs affiliated with hospitals outside the City’s network will be reimbursed per GHI’s out-of-network schedule after a $30 copay.”
These are not hypothetical ideas — they are part of the the original plan design blueprints from at least 2018, if not earlier.
The City and its provider vendors modeled the exact cost-tiering structure years ago.
The only missing step was MLC finally accepting their proposition and implementation.
So when the UFT insists “no tiering,” it’s denying a design already embedded in City planning documents and actuarial projections. The prototype to the actual hospital plan is what we see presently in the NYCEPPO plan.

The Strategy: Lying Through Framing
Here’s how this deception works:
No tiering. Creates comfort and avoids panic.
Option to tier later. Reserves full power for future enforcement.
"Implementation via cost-pressure or arbitration. Converts “option” into policy once members are trapped.
This tactic — framing without falsifying — is why legalistic, biased FAQs are so dangerous. They make sweeping assurances while embedding contractual escape hatches.
We know that the UFT’s paid operatives that helped with this FAQ framing and sold the plan to members are not privy to these internal documents and plan design. But, what do they say now?
To reiterate, we see an almost identical framework being laid down in this current NYCEPPO plan that will take effect on January 1, 2026.
‘The Wire’ Called It Out Early
The Wire / Educators of NYC sounded the alarm before the MLC vote:
“One of the biggest lies in the leadership’s propaganda campaign is that there are no hospital tiers.”
“A third option has been added, creating a tiered structure that can and will be used to penalize hospitals acting in ‘bad faith’ by requiring higher copays at some of the area’s more elite hospitals — like NY Presbyterian and NYU Langone.”
— The Wire: Why UFT Chapter Leaders and Delegates Must Vote NO
The Wire’s reporting also revealed that the NYCE PPO’s self-funded model mirrors corporate cost-containment strategies — putting “cost savings” above member care and restricting networks while shifting risk and costs onto workers and retirees.
Retirees’ Warning: “The Devil Is In The Details”
Marianne Pizzitola, president of the NYC Organization of Public Service Retirees, has fought this same managed care concept in the City’s Medicare Advantage push.
She warns that tiering is the gateway to privatized care restrictions like we find in Health Maintenance Organizations (HMOs):
Once tiering enters the contract language, it becomes the enforcement mechanism for network control — much like we find in any HMO.
Her coalition’s legal victories exposed how insurers weaponize managed care to deny or delay care.
Now, she cautions, the same manage care blueprint is being expanded to active employees under the NYCE PPO.
She’s also warned retirees and active workers about voting to approve a healthcare plan without first reading the terms and conditions in the contract.
Mulgrew is Perfectly Okay With Managed Care
Mulgrew is all in on this type of tiered managed care. His words to the delegates at the September 29th DA confirm how he feels about managed care — with its more restricted networks.
While assuring UFT delegates that there’s no tiering in this new plan, he added:
Do we want a much more inclusive managed care program, which is really a big deal? We have proven this, but at this point in time, we’ve been managing care voluntarily for a lot of our diabetics and different people with different conditions.
We want to expand that, because first of all, it gives you and your loved ones better health care and a better quality of life. And second, it actually saves money, so you got to manage the healthcare.
What Tiering Really Means for Members
Tiering isn’t an abstraction — it’s a cost shift.
Higher copays at hospitals deemed “bad actors, “Tier 3” or even “Out-Of-Network.
Restricted provider choice as physicians get categorized by hospital affiliation.
Penalties disguised as incentives, pushing patients to cheaper understaffed, under-resourced city facilities while punishing those opting to go to more elite, high performing hospitals.
Locked arbitration structures preventing member renegotiation.
The City has already modeled using increased copays as a economic behavior modification technique with higher copays for Emergency Room visits and Urgent Care visits.
Now, the long planned tiering infrastructure is now in place.
All that’s missing is the trigger — rising costs that “necessitate” activating tiers into full throttle.
They will claim to be penalizing the “greedy, evil hospitals”. But, ultimately, we bear the costs out of pocket when they punish “uncooperative” hospitals just as we have with higher copays in recent years.
We shared another 2018 internal document in an earlier post that showed potential scenarios being floated around of copays on elite hospitals like NYU Langone and New York Presbyterian being as high as $2500 (see page 3).
The Bottom Line
The NYCE PPO is tiering, whether they say the word or not.
The UFT leadership’s FAQ regarding tiering is a misleading frame; the 2018 OLR memo proves the intent.
The Wire and Marianne Pizzitola have both sounded the alarm: this is managed-care privatization in union wrapping.
They say there’s no tiering. But it’s already in the paperwork, the contracts, and the plan design. The only thing missing is our consent and this plan to be finalized and enacted.
They knew. They planned it. And they’re counting on you not to notice.
We must organize!
Receipts
City of New York OLR Memorandum, “Questions on Menu of Savings”, Feb 8 2018
Educators of NYC – The Wire: “Why UFT Chapter Leaders and Delegates Must Vote NO”
Internal City Document: Projected 2019 Savings If Changes Made to Our Healthcare
Learn More:
Behind the Gates: How UMR Takes Over Utilization Management In Our Health Plan — and Why the AI & 'Clean Claim' Clauses Should Sound Alarms

Meet United Medical Resources (UMR). They’re not a household name, but under the new NYCEPPO plan, UMR will become the central authority deciding what care you can and cannot get. Acting as the Third Party Administrator for UnitedHealthcare and Emblem, UMR will be the interface every member has to go through for nearly all preauthorizations, claims, and…
Thank you for your dedicated reporting Daniel. While It's hardly any comfort that this validates how you and others kept warning members about NYCE PPO's tier hospitals, as you say, we should use what's coming out to organize!
And they will freeze provider reimbursement rates.